Conditions I treat......... Flat feet
Non-operative treatment of flexible flat feet
Flexible flat feet are very common in the normal population and generally don't cause too many problems in young patients. However, as children pass through the teenage growth spurt, problems can arise. Calf muscles can become tight and act as a deforming force on the heel. In teenage years, children tend to get heavier. Both factors can lead to a previously symptom free flat foot becoming a bit stiffer and uncomfortable when walking long distances.
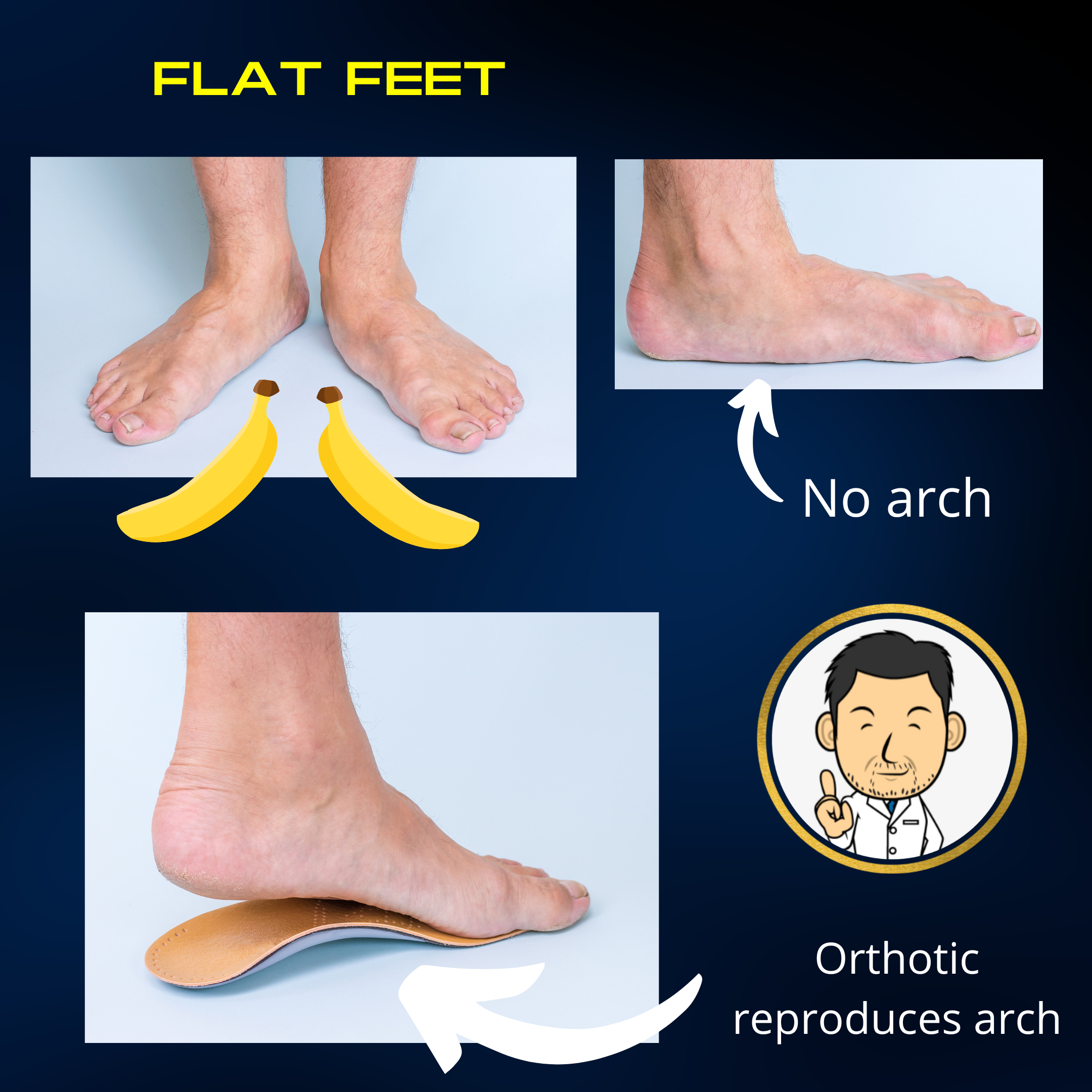
The initial treatment of symptomatic flexible flat feet is always non-operative as in the vast majority of cases this will be sufficient to ease symptoms. A good insole/orthotic can help augment the medial arch and push the heel straight making walking longer distances more comfortable. Physiotherapy to stretch out the calf muscles also makes the flat foot more supple and comfortable. A good foundation of non-operative treatment is essential before embarking on any plans for surgery.......
Surgery for symptomatic flexible flat feet
Surgery for symptomatic flat feet is only indicated in a very small minority of patients with flexible flat feet who still have persisting symptoms despite an adequate course of non-operative treatment. Usually these are teenagers with quite marked flat feet who have done well initially with insoles but over time found that they still have residual discomfort that they are unhappy with.
There are many different surgical options in treating flexible flat feet including subtalar implants and hindfoot fusions. Subtalar implants enjoy varied popularity amongst surgeons and patients alike due to the minimalistic nature of surgery. A small bullet like implant is inserted via a small incision between the bones in the hindfoot to make the heel straight). Unfortunately, these implants can give rise to pain over time and often will require a second procedure to remove the implant. A hindfoot fusion straightens the heel by fusing the joint between the ankle bone and the heel bone. Issues can arise when stresses are transferred to neighbouring joints causing them to problems in later life. Generally, it is best to avoid fusing joints in children's feet if alterantive treatment strategies can be employed.
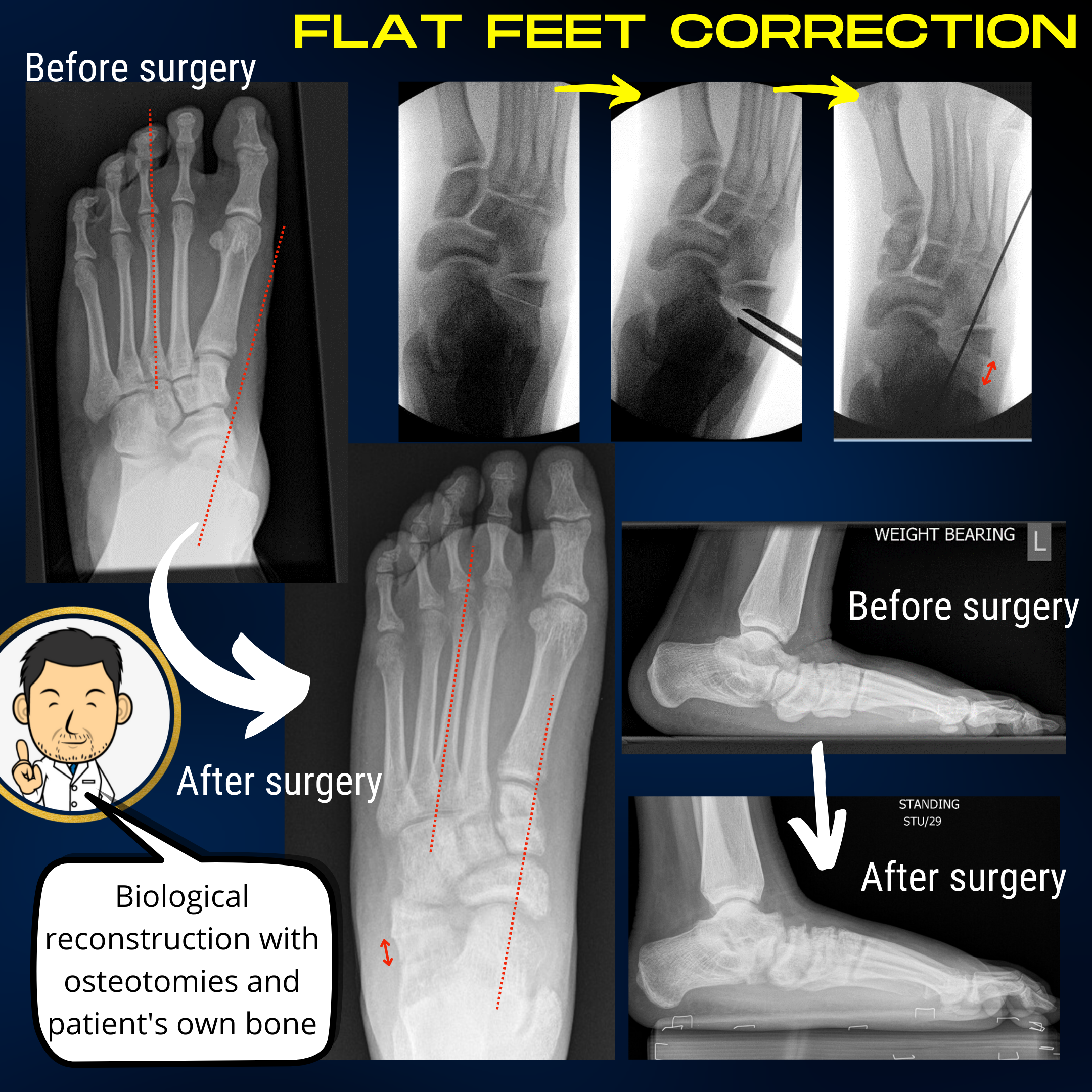
My preference is to undertake a biological reconstruction of symptomatic flexible flat feet. The operation entails changing the shape of specific bones to re-align the foot when viewed from above and the side. Bone taken from the pelvis of the same patient is used to augment the foot's bony architecture alongside soft tissue procedures to re-balance the muscles acting on the foot. It is an a la carte approach with specific procedures tailored to the patient's specific deformity. I received instruction in this surgery during my fellowship in Sheffield Children's Hospital. Seeing the operated patients at follow up convinced me that this is perhaps the most effective (and safest in terms of long term outlook) procedure to do on symptomatic flexible flat feet. I usually wait until skeletal maturity when the foot has completed most of it's growth before embarking on this surgery to minimise the risk of a recurrent deformity with further growth.
It is important to stress that flat feet are generally the norm in children and do not require treatment unless symptomatic. Only a small proportion of children with significant deformity will develop problems and this is usually in adolesence. The vast majority of these will respond to simple measures such as orthotic insoles and physiotherapy. Surgery is therefore reserved for a very small minority of patients who have intrusive symptoms despite these non-operative measures. This message can not be over-emphasised as the treatment of the asymptomatic flat foot in children is a vast economy in which custom made insoles are continually prescribed in the absence of any evidence supporting their benefit.
Treatment of rigid flat feet
This is a bit more challenging as rigid flat feet usually denote an underlying disorder and/or are the sequelae of previously surgically treated feet.
Congenital vertical talus
A very interesting condition which exists on a spectrum ranging from a flexible deformity (the oblique talus) to a complete irreducible dislocation. The deformity may be present at birth or manifest itself in the first few years of life. When approaching any little foot, my strategy is the same - serial casting to correct the deformity until no more benefit can be derived. The point I hope to reach is where the remaining deformity can be addressed with procedures that will not compromise future foot function - usually temporary pinning in cast, tendo achilles tenotomy and tibialis anterior tendon transfer. In cases of fixed dislocation (usually with a syndromic basis) more may be required but serial casting to ad infinitum (or thereabouts) is always the pre-requisite before making this judgement.
Tarsal coalition
Tarsal coalition is an abnormal bony connection between two independent bones in the foot. There are two principle locations - the calcaneo-navicular coalition and the talo-calcaneal coalition.They frequently affect both feet, can be an incidental finding and have no clear consensus on optimal treatment. The theoretical benefit of surgically removing the coalition to restore movement in the joint is frequently obviated by the fact that the joint remains stiff thereafter. In patients with specific symptoms, excision of the coalition (removal by surgery) may have a role but outcomes can prove unpredictable. Often the alignment that the foot has stiffened into can be just as much of an issue as the coalition. Best approached on a highly individualised basis.
Spina bifida
Paralytic disorders are amongst the most challenging conditions to treat in Pediatric Orthopedics. In essence, a permanent deficit in certain muscle groups leads to a permanent deforming force which progressivle deforms the bony anatomy of the foot. The loss of protective sensation in the foot adds further challenges in treatment. Surgery may have a role in specific patients but best assessed on an individual case basis.