Conditions I treat......... Guided growth for angular deformity in growing children
The term "game-changer" is vastly mis-applied in current times. For example, a popular fast food chain will come up with a new burger and market it as a "game-changer." It may have a new brand of cheese or some bizarre inclusion (Cheetos spring to mind). But at its heart it will still be a patty between two bits of bread. This would not constitute a sufficient deviation from expectation to qualify as a "game changer." However, guided growth in the management of childhood deformity has been just that - a true "Game Changer." Before the advent of this technology, to correct a bent bone there was no option but to break it. Once straightened, it had to be fixed in place with a device, usually a metal plate/rod/nail. We then had to wait for the bone to heal before allowing the child to return to normal physical activity.
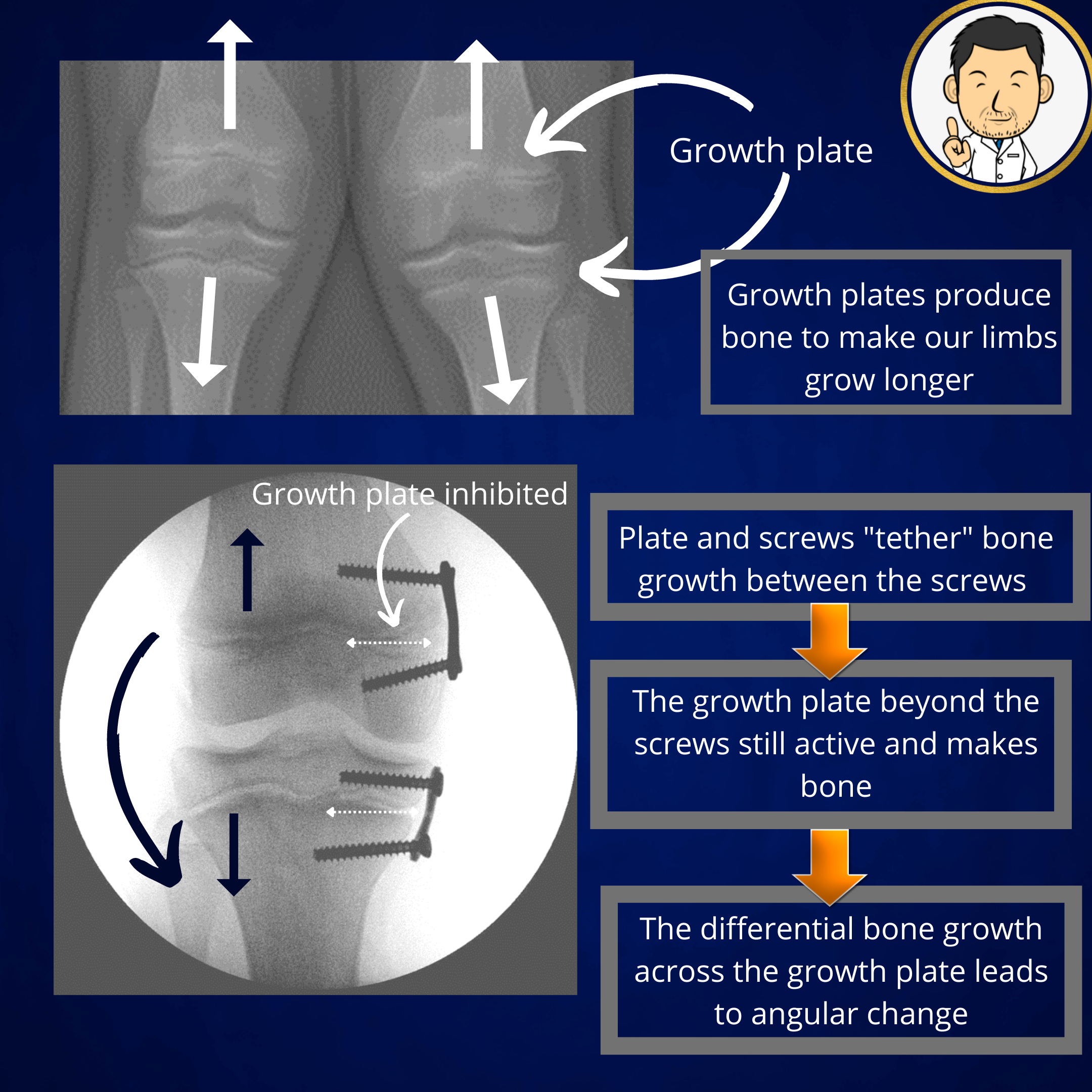
But then guided growth came along..... and the rules of the game changed. This time the bone didn't have to be broken. The scale of surgery was vastly reduced to placing a small plate in a crucial location on the bone. We only had to wait for the skin incision to heal. The patient could walk on the day of surgery and get back to physical activity as soon as they were comfortable. Over time as the child grew, the deformity would correct. Incredible but true.
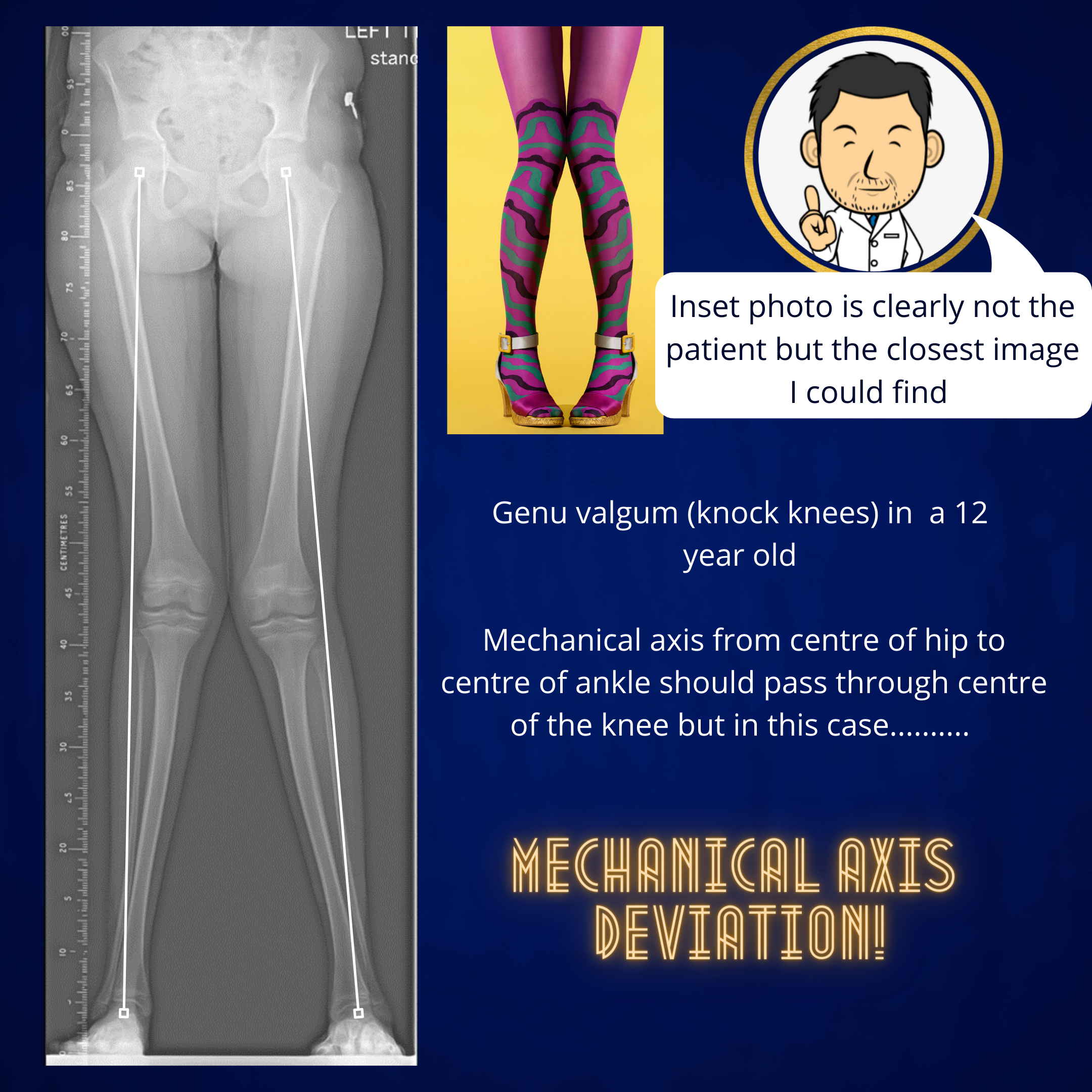
So how does it work..... Technically, the plate acts as a tension-band across one side of the growth plate (the cartilage region at the ends of long bones which pushes out bone to make the limb longer). A tension-band implies a "band" that doesn't stretch (because the plate is made of metal and the growth plate isn't powerful enough to stretch metal). The metal plate-screw construct envelops the growth plate - effectively "tethering" growth on one side of the bone as the growth plate can no longer push out new bone. However, the growth plate on the other side of the bone opposite the plate is free of this "tethering" influence and can still push out new bone......
This means that with further growth, a differential is set up where the length of bone doesn't increase on the "tension band" side but does increase on the other side. This differential growth brings about angular change to correct the intended deformity. The pre-requisites are that the growth plate is healthy, sufficient growth remains and the magnitude of deformity correction is within reach of what the technique can achieve. Often, guided growth may not give us the complete solution we require for deformity correction but any help it gives us in reducing the extent of future surgery can only be a good thing.
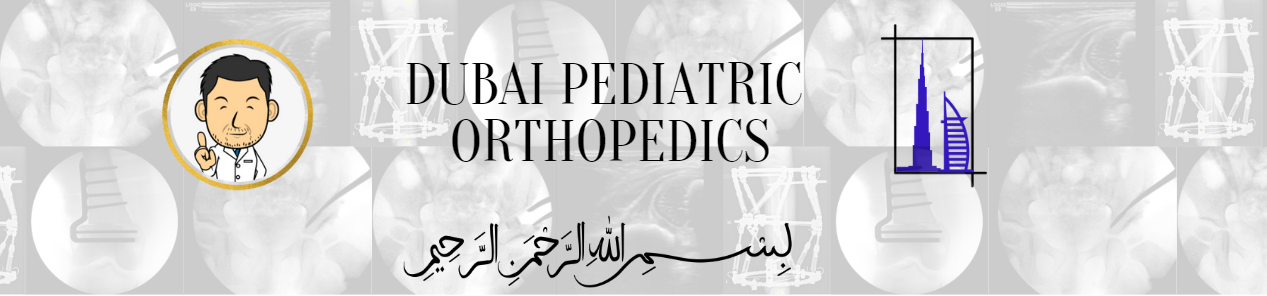
Time for an illustrative case....
So what happens if the plate is left in after the desired correction has occurred? Not a lot if the patient is close to completion of growth. Towards the end of growth the growth plate pushes out gradually less and less bone (evidenced by a narrowed appearence on x-ray) and eventually disappears, completely replaced by bone. In such cases the plate is no longer active and can remain inside the patients if not giving rise to any localised symptoms. However, if there is still growth remaining after the correction is complete, the plate is still "active" and angular change will continue.........
If there is growth remaining after the desired correction is achieved, the plate's effects can be negated by removing the plate and screws. However, with further growth there can be a "rebound" phenomenon where the bone over-reacts to the plate's absence and pushes the bone back towards the original deformity. Another operation to implant a new plate to restart "guided growth"seems quite arduous. If only there was some way to "de-activate" the plate without removing the whole construct....
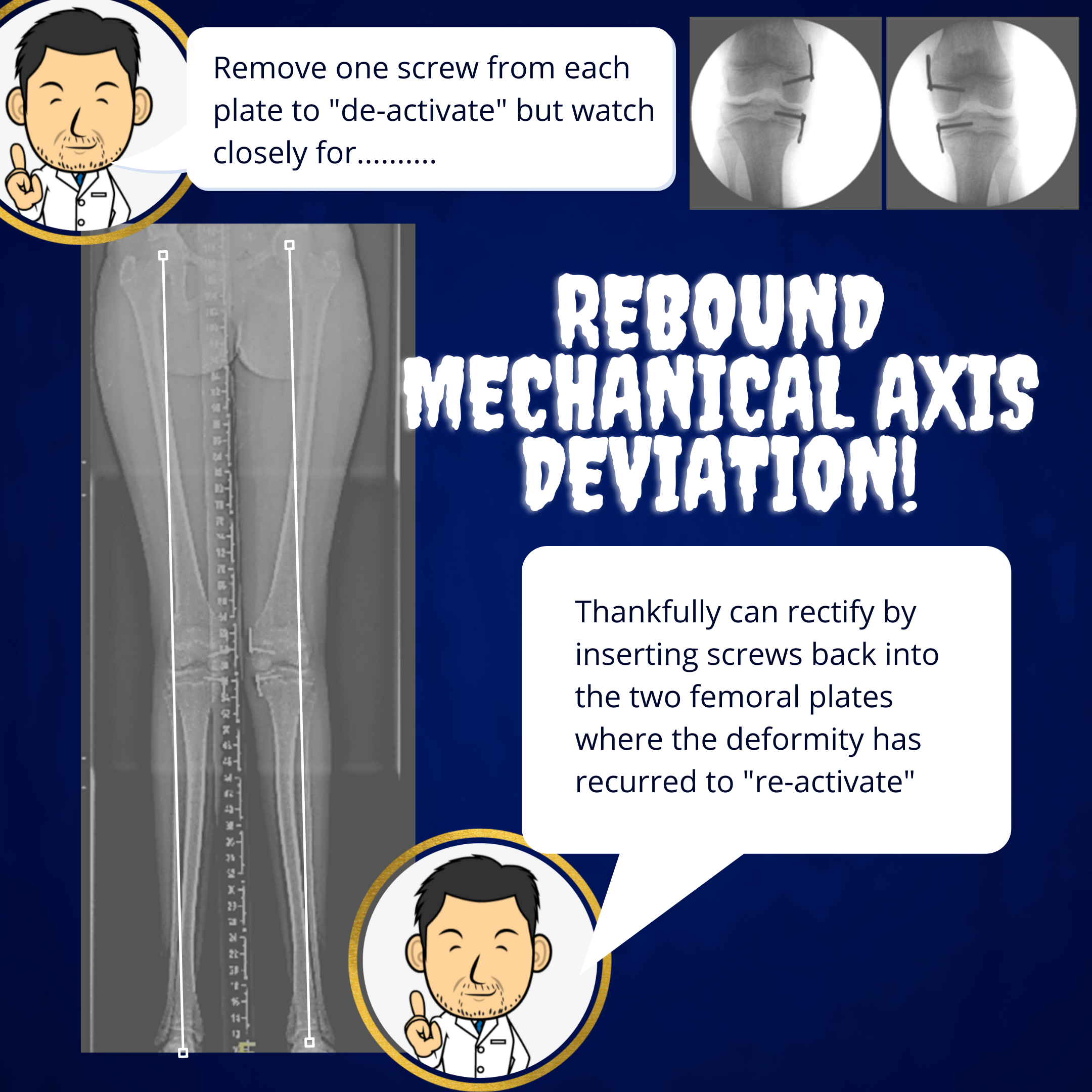
Thankfully, " guided growth plate de-activation" is very much a thing. Removing just one of the screws from the plate (not the one adjacent to the joint as this is more fiddly to re-insert) is sufficient to remove the "tension band" effect. Then, if there is a "rebound" phenomenon, re-inserting the missing screw "re-activates" the plate. I have described the dormant plate as being temporarily "de-activated" which I think is perhaps an appropriate descriptor. Other surgeons have labelled this as a "hibernating" or "sleeper" plate but the concept is exactly the same and needless to say that I didn't come up with the idea first. However, I have found that I can't easily get away with a discussion involving "activating sleepers" without raising more than a few eye-brows
Usually it's best to leave guided growth as late as possible to avoid having to continuously play a "cat and mouse" game of de-activating and re-activating a plate with further growth. Usually after the age of 10 years is fine for correcting uncomplicated genu valgum or varum (bow legs and knock knees). However, conditions like Blounts or growth plate dysfunction may mandate deformity correction with guided growth at an earlier age.