Conditions I treat......... Limb reconstruction : Deformity correction with internal fixation
Hip reconstruction
In most cases of congenital longitudinal deficiency (leg shortening present at birth due to reduction in length and constituent elements), addressing any joint distortions merits equal consideration to correcting shortening of the limb.
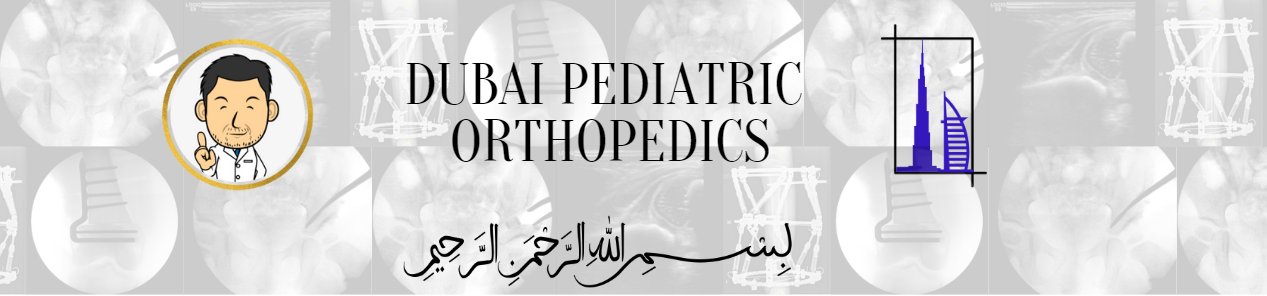
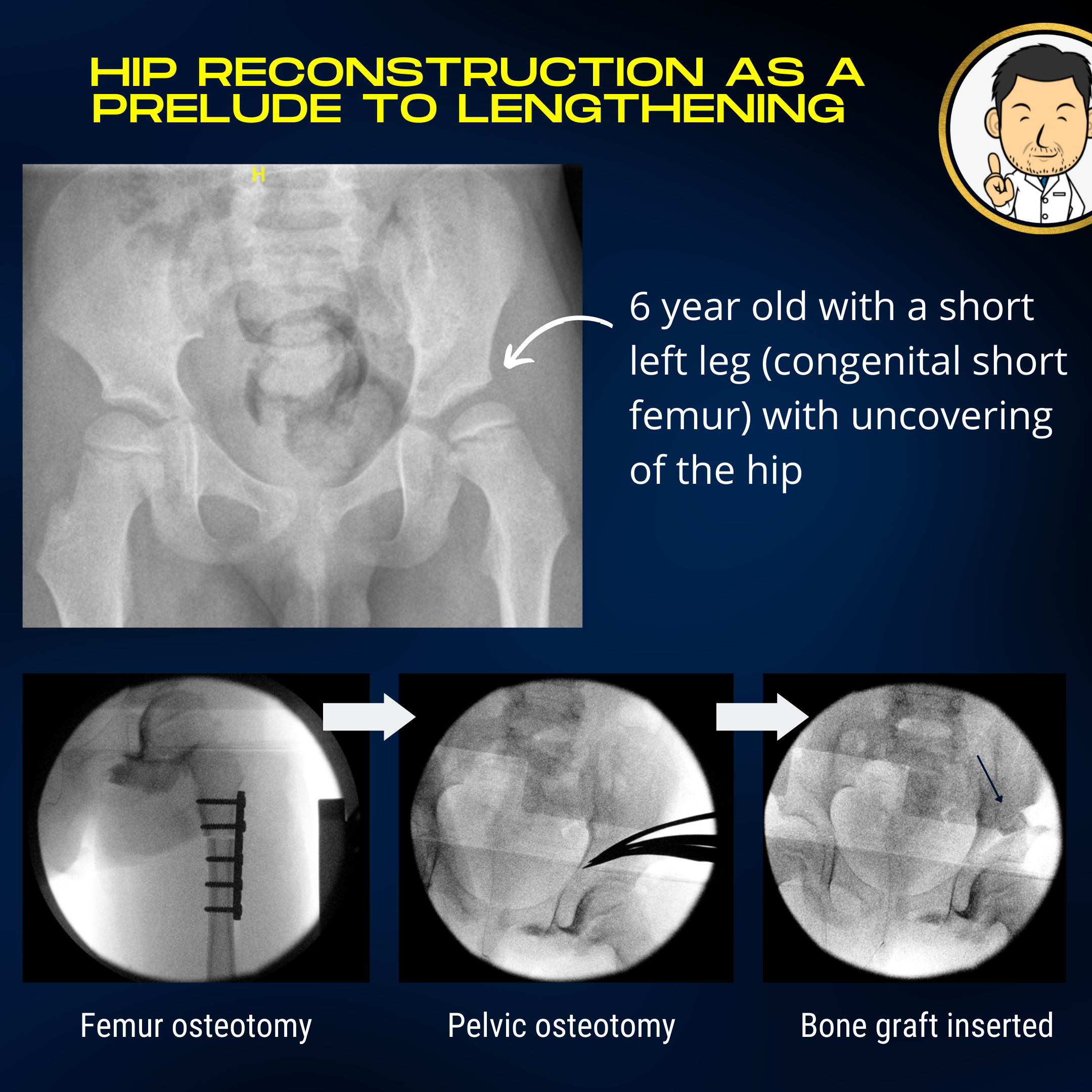
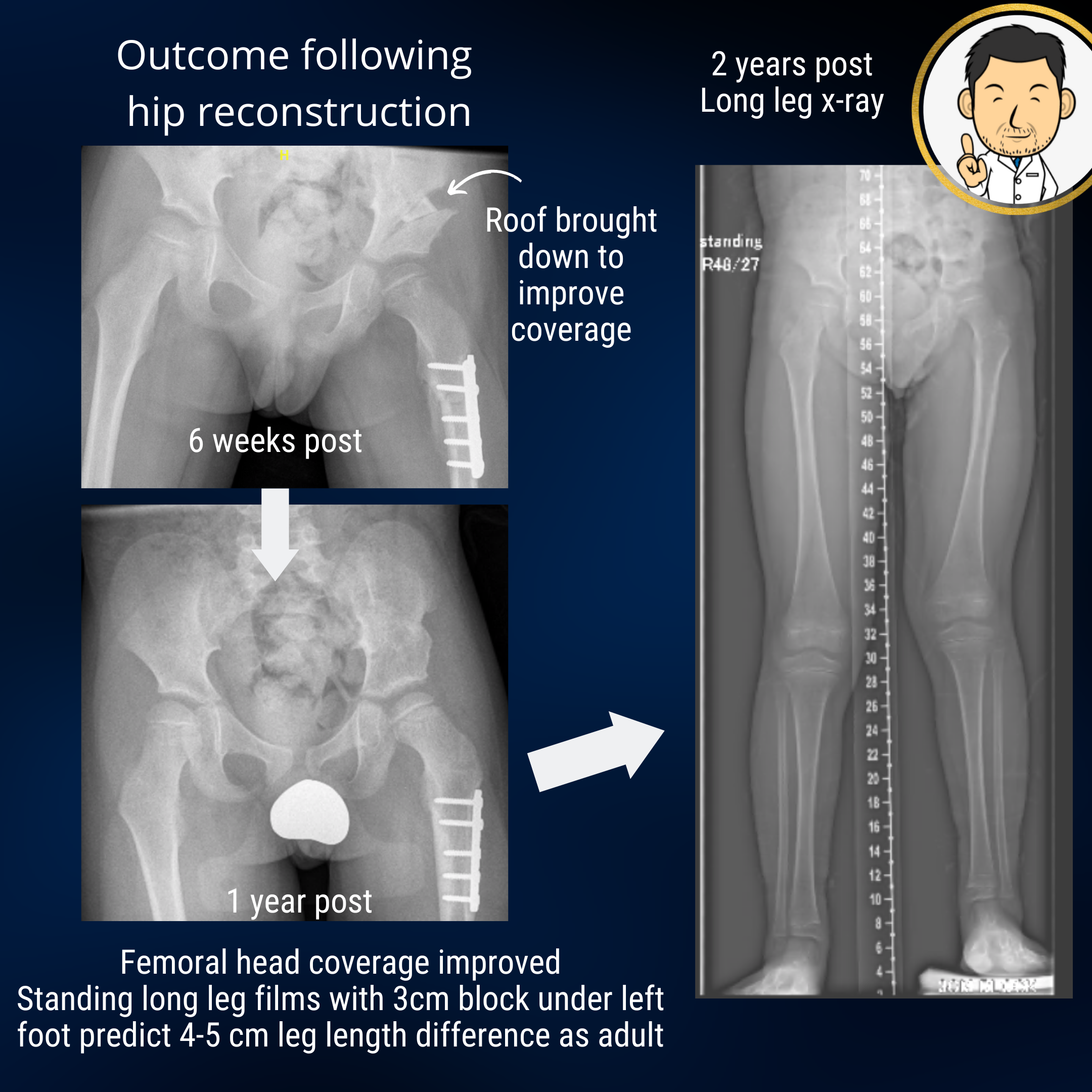
Proximal focal femoral deficiency is a congenital longitudinal deficiency predominantly affecting the femur. The mildest variant is the congenital short femur where mild femoral shortening may be accompanied by mal-alignment of the hip joint. The top end of the femur may have a "crooked hunched over" appearance and the socket may be shallow. Although, shortening in itself produces an asymmetric gait, the abnormal hip anatomy often leads to an "out-toeing" walking pattern with early fatigue due to muscle inefficiency. The socket may be shallow. If left unaddressed, this may lead to the hip dislocating if the femur is lengthened when the child is older. Correcting the alignment of the hip joint and improving socket coverage are goals that should be addressed early. The "surgical footprint" (a euphemism of the magnitude of surgery and it's impact on the patient) is much less when the hip is reconstructed early in life compared with when the child is in their teens. Early hip reconstruction improves the outcomes and risk profile of later limb lengthening surgery.
Knee alignment correction
In growing children, guided growth is an excellent means of tailoring growth to correct angulatory deformity around the knee. In older children, there may be insufficient remaining growth to enable such a correction. Thus, the only option is to divide and re-allign the bone to achieve the desired correction. When both angulation and length correction are required, a circular frame is often the best device. However, if the deformity is purely angular with no length considerations, correction and internal fixation with a metal plate may be the more desirable option (as stated elsewhere, "a frame is the most appriopriate option when a frame is the only option"). The clear advantage is that the fixation is all on the "inside" which is vastly less intrusive to the patient.
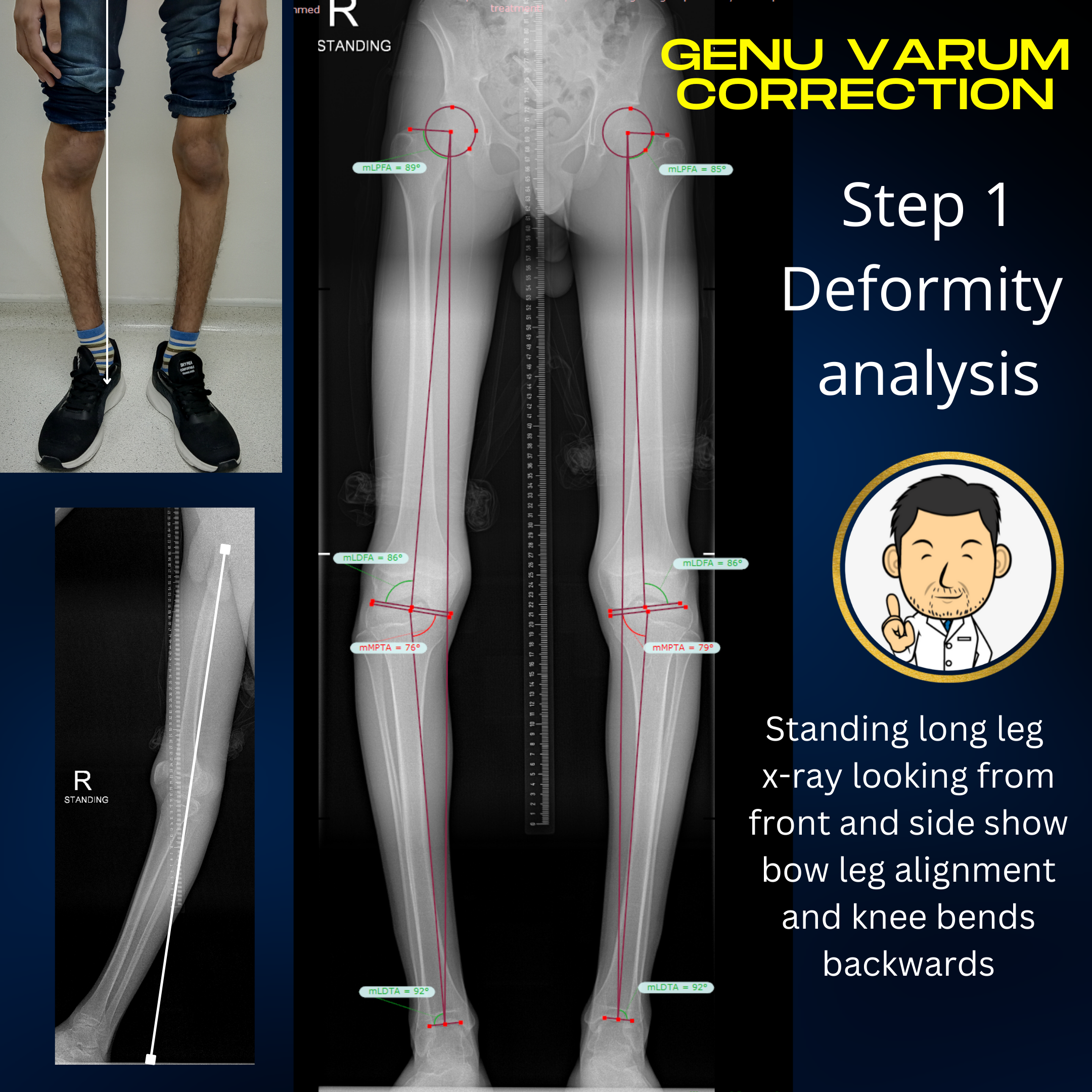
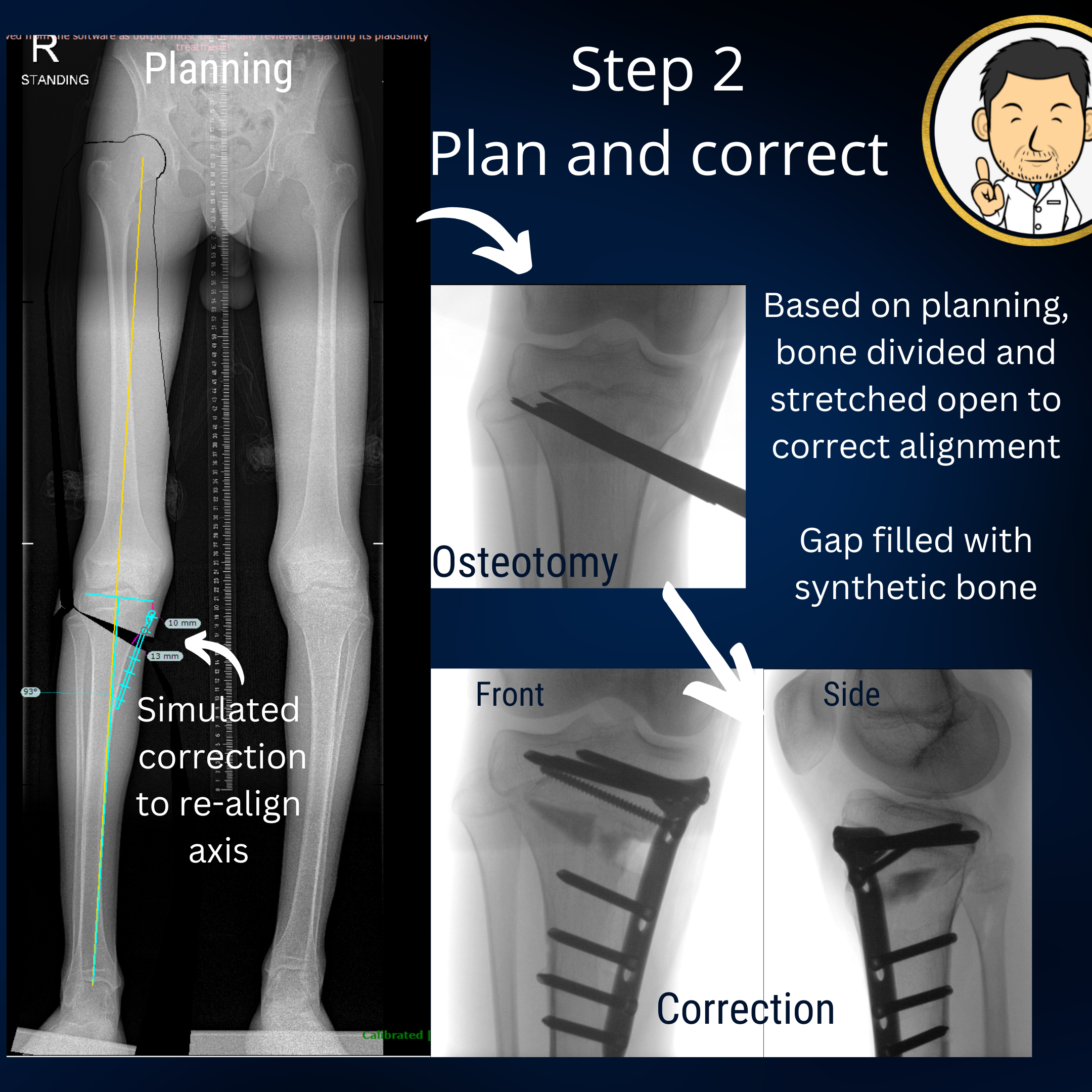
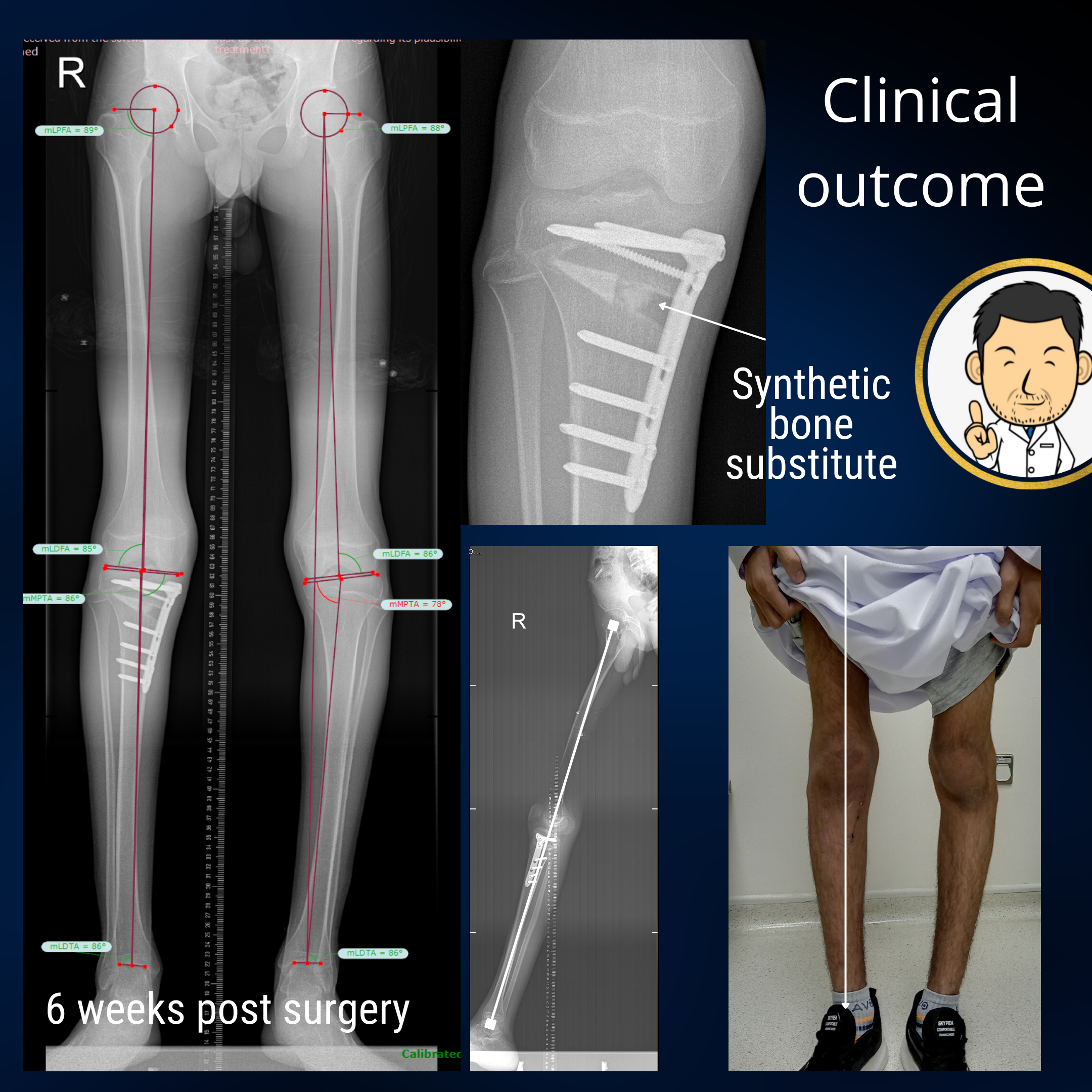
A common pattern of deformity at the knees is "bow legs" due to an oblique plane at the top of the tibia (shin bone). This is often coupled with a knee which hyper-extends (bends backwards). A carefully planned osteotomy creates an opening wedge in two planes to correct both deformities. Fixation with a plate internally is a true blessing for patients compared to treatment with an external fixation. I instruct patients to be non-weightbearing for the first 6 weeks. If all is good on the x-ray at 6 weeks, they can progress to full weight bearing thereafter. Usually I do one leg at a time so the patient can remain relatively mobile throughout treatment.
Ankle correction
Generally the ankle is a lot more permissive for angular deformity than joints upstream. However, occasionally a situation demands that an angular correction needs to be undertaken. If there is no lengthening required, then correction with internal fixation may be feasible.
Rotational correction
The rotational alignment of the lower limbs has a broad spectrum encompassing normality. A deformity has to be well and truly two standard deviations away from normal (a statistical expression of unarguable deviation from normal) before considering surgical correction. Despite their infrequence, such cases do occur. For example, the child with external tibial torsion, out-toeing gait and marked flat feet where correction with growth is not a reasonable expectation. Or the 12 year old child with clown like appearance of moderate to severe in-toeing due to internal tibial torsion. In such cases with severe deformity and functional impairment where the capacity for natural correction has been exhausted, there is a role for surgical correction. However, to put things in context, 5 years of independent practice and thousands of patients later, I have only done this operation in a few children. Troublesome rotational deformities are more commonly encountered in children with cerebral palsy. Here the rotational deformity is but one element of a far more complex deformity pattern which needs to be corrected.