Conditions I treat......... Slipped Upper Femoral Epiphysis (SUFE)
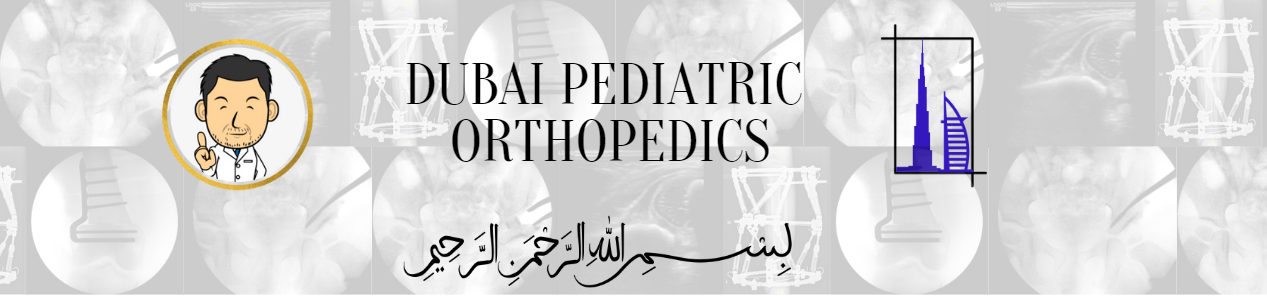
Pinning in situ for mild slips
In Slipped upper femoral epiphysis (SUFE), the femoral head (ball) has tipped off the neck through failure of the growth plate interface between the two. If the slip is mild (i.e. anatomy is not too distorted) further migration of the femoral head can be arrested by passing a screw across the growth plate. Often, the residual deformity is mild and with growth smoothes out through a process known as bone remodelling.
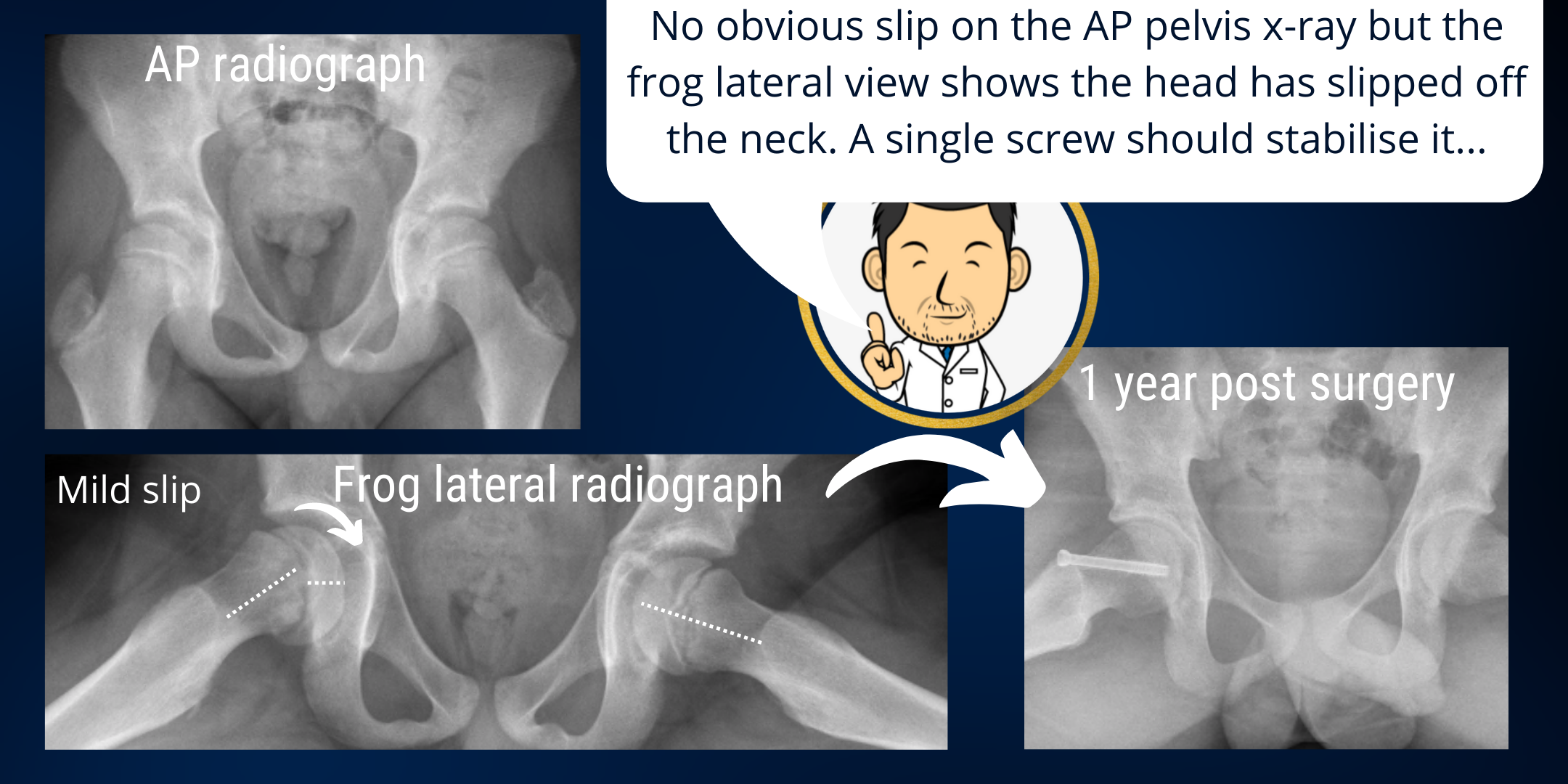
Intracapsular osteotomy for acute deformity correction
When a severe slip occurs it may do so slowly (often over many weeks or months) or suddenly (usually after an accident). A sudden (acute) severe slip is a very bad prospect as there is a significant risk of the blood vessels to the femoral head being damaged causing progressive necrosis and collapse of the femoral head with early arthritis. In such instances, both the severe deformation of the anatomy and its unstable nature threatening the blood supply need to be addressed. This is usually done by surgery to open the hip, shorten the femoral neck to detension the neighbouring blood vessels and then place the femoral head back on. The femoral head is usually stabilised with two screws. Despite optimal treatment there is a significant risk of the blood supply to the femoral head being compromised and patients and their families need to be counselled appropriately.
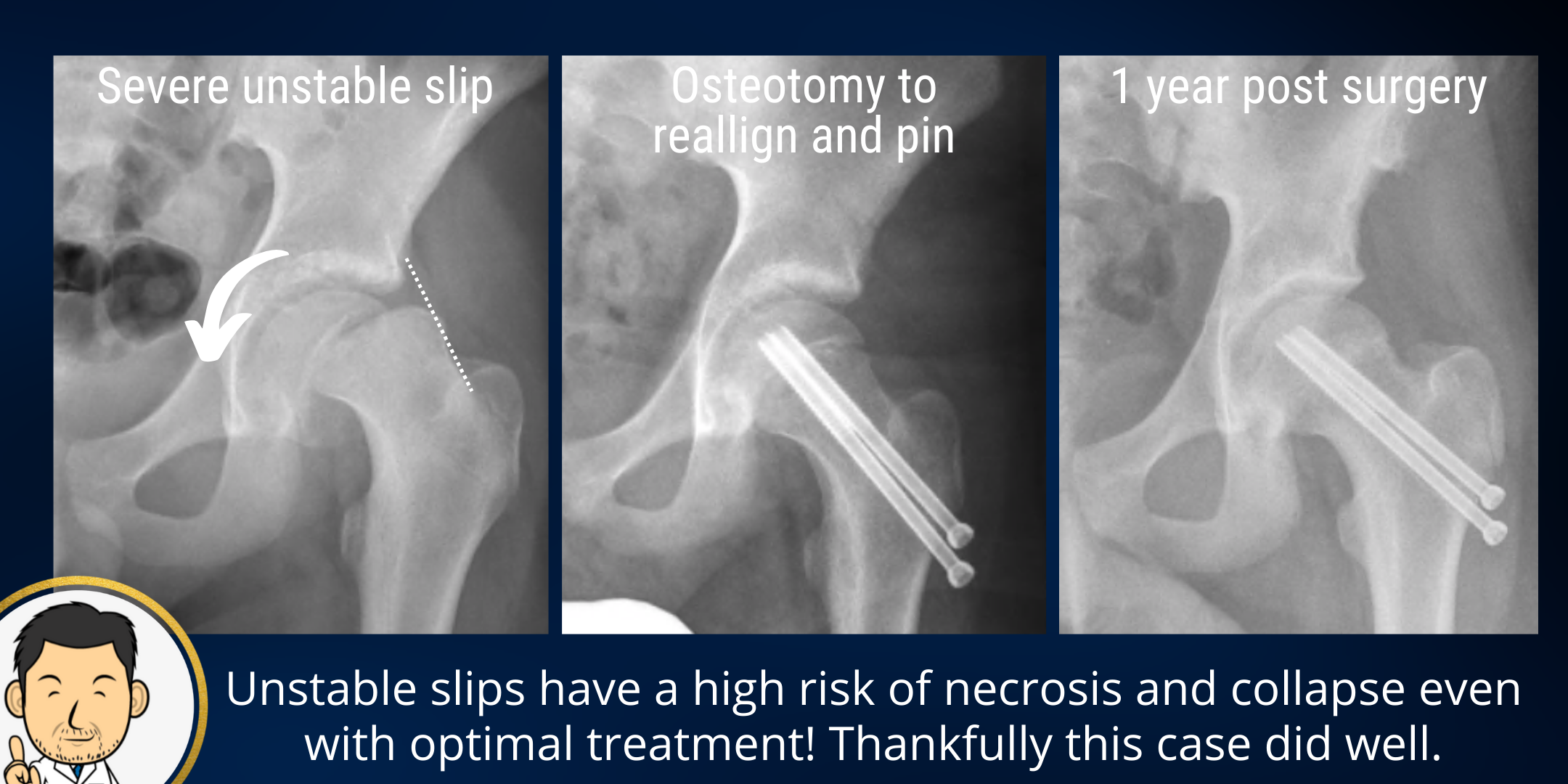
Pinning in situ for severe stable slips
Sometimes a slip takes place over a long time - almost in slow motion. As the femoral head slips off, adaptive changes in the bone smooth out and compensate for the deformity. Often these patients present with background pain for some time. Two issues arise - (1) whilst the growth plate is open, the femoral head can keep on slipping and (2) the more severe the magnitude of the ongoing slip, the greater the deformity in the femoral head. There are good studies to suggest that the distorted anatomy resulting from a severe stable slip will eventually lead to degenerative change in the joint and painful arthritis. Therefore even if the hip stops slipping, the deformity it has created can not be left untreated.
My favoured approach is to arrest the slip with a single screw. This stops the slip getting any worse and also helps ease the pain associated with the instability. The deformity in the femoral head can be addressed once growth is complete and the anatomy is static. Therefore these patients do need follow up to completion of growth when further surgery can be undertaken to correct the deformity.
Deformity correction for severe stable slips
Often there are several deformities which need to be addressed in the chronic slip. There's usually a deformity in two planes (in actuality it's the same deformity but on an oblique plane.....) as well as an added rotational element. Left untreated severe stable slips do manifest arthritis in later life. My preference is to correct the deformities in the femoral bone away from the joint (and the crucial blood vessels supplying the femoral head). The femoral osteotomy enables angular correction in both planes as well as correcting the rotation.